
 Traditional health practitioners and government working together
Traditional health practitioners and government working together
By John De Coninck, The Cross-Cultural Foundation of Uganda
(see below for the french summary)
The status of traditional medicine
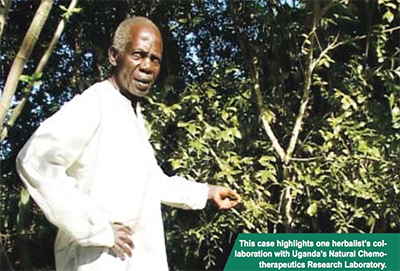
More than 60% of Uganda’s population depends on traditional medicine because it is accessible, affordable and culturally familiar. With an estimated traditional health practitioner for every 200-400 Ugandans (compared to 1 western- trained doctor per 20,000), herbal medicine has long been used to manage a range of common conditions, including malaria, digestive and respiratory problems, toothaches, skin diseases, and childbirth complications. This document examines the relationship between Uganda’s Ministry of Health and a traditional herbalist, its strengths, challenges and its implications for future policy. The Cross-Cultural Foundation of Uganda worked with the Natural Chemotherapeutics Research Laboratory (NRCL) and a herbalist, Hajji Zakariya Nyanzi, to prepare these pages.
NCRL identified Hajji Nyanzi, a farmer and traditional health practitioner in Mubende district, as exemplary because of his experience, willingness to share information and long standing collaboration with NCRL, the AIDS Support Organisation (TASO) and THETA, the Traditional and Modern Health Practitioners Together against AIDS and other diseases.
The emerging policy framework
Until recently, there has been only limited recognition of the contribution made by Uganda’s traditional health practitioners to primary health care. This is in part because of the colonial legacy, during which culture was branded as negative and primitive (The 1957 Witchcraft Act outlawed traditional medicine and is still on the statute books), and in part because of an education system that rarely values local knowledge. Efforts are however now being made to promote traditional medicine. The NCRL Director, Dr Grace Nambatya, notes that Government’s current interest can be traced back to a 1987 Health Sector review, which revealed Uganda’s limping health care system. In spite of this, an invisible hand seemed to be at play, as the health status of Ugandans was not as disastrous as expected: traditional healers were then identified as a key contributor to primary health care. It was therefore recommended that they be brought into the mainstream health sector.
The Ministry of Health in time opted for a public-private partnership in which traditional health practitioners would be recognised as private partners. More recently, a new policy on Traditional and Complementary Medicine has been drafted to regulate the practice of traditional medicine, to focus on research and development and to encompass protection, cultivation, propagation and sustainability of traditional medicinal plants.
The Ministry has also submitted a Bill for the establishment of a semi-autonomous body, the National Council of Indigenous and Complementary Medicine Practitioners, to support collaboration between the “modern” health sector and traditional practitioners and to regulate the latter, while protecting their intellectual property rights.
 Working with the Natural Chemo- therapeutics Research Laboratory
Working with the Natural Chemo- therapeutics Research Laboratory
The Ministry of Health started to promote research and conservation of medicinal plants with the establishment of the NCRL in 1963. At the time, however, efforts to verify and authenticate traditional medicinal products were in part constrained by the absence of well-established associations of traditional medicine practitioners.
Today, traditional healers have formed associations to represent their collective interests. NCRL provides financial and technical support to practitioners to identify medicinal plants, and to assess the efficacy and toxicity of their herbal medicines, following established standards. Once validated as safe for human consumption, a healer’s product is recorded as such, and the healer is encouraged to have his product notified by the National Drug Authority (NDA).
After notification, herbalists are required to track and to submit further information on the safety and effectiveness of their products, before registration with the NDA. NCRL gives them advice on these procedures and on expanding the production of medicinal products, where appropriate.
It may itself process and package selected medicines as prototype samples. NCRL also offers training to practitioners through their Associations in herbal garden management and conservation, processing and packaging (including labelling with expiry dates), hygiene and protection against HIV/AIDS. Traditional healers, on their part, provide information on herbal medicine and practices, and share detailed information on the medicines that have proven effective. This contribution is acknowledged on the labels of herbal medicines samples packaged by NCRL.
 NCRL has undertaken considerable research to transform raw herbal products into validated, registered, well-packaged and labelled medicines: by the end of 2007, 80 products had been notified as safe and effective for public consumption. With positive findings on the effectiveness of traditional herbal medicine on malaria and HIV opportunistic diseases, the World Health Organisation is currently funding further research in this area through NCRL. With training, the quality and presentation of herbal medicine has also improved, thus providing healers with better income. Dr Nambatya also points out that NCRL has come to appreciate the healers’ approach to health care: not only do they apply remedies, they also diagnose holistically, referring to the patient’s psychology and social, natural and cultural environments.
NCRL has undertaken considerable research to transform raw herbal products into validated, registered, well-packaged and labelled medicines: by the end of 2007, 80 products had been notified as safe and effective for public consumption. With positive findings on the effectiveness of traditional herbal medicine on malaria and HIV opportunistic diseases, the World Health Organisation is currently funding further research in this area through NCRL. With training, the quality and presentation of herbal medicine has also improved, thus providing healers with better income. Dr Nambatya also points out that NCRL has come to appreciate the healers’ approach to health care: not only do they apply remedies, they also diagnose holistically, referring to the patient’s psychology and social, natural and cultural environments.
Hajji Zakariya Nyanzi
A herbalist of many years’ experience, Hajji Nyanzi has consolidated his knowledge and practice by joining various groups promoting traditional medicine: first a local association, the Kitalegelwa Group of traditional healers, then THETA, where his medicine for malaria was assessed, processed and packaged for distribution to the public. He also joined Uganda N’eddagala Lyalyo, a national association of traditional healers, where he learnt about other opportunities to improve his herbal medicine, and was advised to take his products to the NCRL for assessment.
Hajji Nyanzi currently supplies herbal medicine to patients within and beyond his community, as well as to NCRL and THETA. Hajji Nyanzi produces herbal medication in powder and liquid form for malaria, fibroids, and some HIV/ AIDS-related conditions (commonly locally referred to as ‘kadomola’ [jerry can]), among others. These have been used by his patients for some years, according to him, to good effect. NCRL and THETA have singled out his remedy for malaria as most effective. NCRL has trained Hajji Nyanzi in processing and packaging herbal products, in protection against HIV infection, and in managing herbal gardens. The Laboratory has sent some of his products for notification, including for malaria and fibroids, and Hajji Nyanzi is in the process of registering some of these with the NDA.
He welcomes the tests carried out by NCRL and feels these add value and market appeal to his products. The Laboratory packages and sells some of these products, and monitors patients taking his medicine. It also links Hajji Nyanzi to these patients so that they discuss progress or any challenges faced. NCRL pays him for medicines supplied at an agreed price: Ushs 30,000 per 750 grams of his herbal medicine for malaria, for instance. Although not formally contracted by NCRL, the Laboratory recognises his contribution by providing him with some funds to manage his medicinal establishment and to train other healers. In addition, NCRL staff visit him, make reference to his work and refer national and international visitors to him for learning and exchanges.
A challenging relationship
While the linkage between Hajji Nyanzi and NCRL has presented opportunities and benefits for the parties involved, it has also highlighted challenges. First, production costs are high, including the local authority’s licence to harvest medicinal material from the forest. This involves a long search for plants, carried out on foot or using a bicycle when ferrying bulky items. Hajji Nyanzi uses simple equipment to process his medicine, mostly wooden mortars and pestles.
After processing, his products are stored in plastic containers and used bottles, for sale. He has opened several retail outlets in the region, but all closed down because of mismanagement, weak supervision and dishonest shop attendants. Applying the skills acquired from NCRL for drying and packaging herbal medicine is costly, he says – at least Ushs 2 million to buy the necessary equipment – a sum beyond his means.
Despite NCRL’s inability to do so, Hajji Nyanzi expects to be generously financed, as he suspects that the Laboratory is generating much income from his intellectual property. This would include support to purchase the equipment he needs, justified by his long- standing relationship with the institution and the successful validation of his medicine. Hajji’s also regrets that his link with NCRL is not formalised by a letter, memorandum of understanding, or identity card. This, he feels, is necessary for his credibility, beyond his name on package labels, and to distinguish him from practitioners who are not linked to the Laboratory and whose products have not been validated.
 Learning beyond the individual relationship
Learning beyond the individual relationship
This individual case underlines three observations of broader relevance: A policy vacuum – The current legislation to promote and protect traditional medicine is outdated. The process of policy development has been slow, owing to low prioritisation of traditional medicine in the health sector, limited finances, and insufficient advocacy to make traditional medicine, its benefits and opportunities visible.
Such a vacuum results in several constraints: first, negative perceptions of the value and quality of herbal medicine are perpetuated in the absence of effective quality control and regulation of traditional practitioners’ practice, especially since abuses, including human sacrifices, are known to exist. A second constraint concerns the protection of intellectual property rights. Partly because they have been disregarded – even repressed – during the colonial and post-colonial periods, traditional healers are suspicious of the motive of those who have now rather suddenly developed an interest in their knowledge. A limited understanding of patenting and intellectual property rights also intensifies a reluctance to disclose knowledge, for fear of exploitation and that this may be ‘stolen’. Thus, according to Hajji Nyanzi, a number of traditional practitioners are still secretive about the contents of their medicine, resulting in indigenous medicinal knowledge remaining concealed, and some effective medicines not being validated or produced on a large scale.
NCRL staff also report that a healer may grow suspicious half-way through a validation process and then withhold some information or withdraw entirely. Similarly, although the NDA is charged with the responsibility of registering products, a fear persists among healers that neither this process nor liberal trade policies provide any assurance that their knowledge will be safeguarded or that they will benefit, should this be utilised by an investor. Registration is also a lengthy, centralised process that requires follow-up in Kampala. This can be costly for traditional practitioners who often live far away and cannot afford to travel to the city regularly.
Patenting is then perceived as suitable for commercial traders in or near the city centre. A third constraint concerns environmental protection. Herbal gardens can provide easy access to medicinal plants, can help to preserve rare and commonly used species and to conserve the environment, in addition to creating employment for traditional healers and small farmers. Herbal gardens and cultivation of rare medicinal plants are therefore essential if benefits are to be sustained. Policies to promote and protect medicinal plants, such as through controlling the felling of trees with medicinal value for construction or charcoal, are currently inadequate. Other policies, such as on agricultural zoning, farmer cooperatives and commercial farming, could also be adjusted to ensure the sustainability of medicinal plants.
Income generation, quality and public-private investment – Traditional herbal medicine is used by a large percentage of our population and provides a potential source of household income. It is therefore in the interests of traditional healers, development workers, health workers and the private sector to promote the production of quality herbal medicine. Once medicine has been validated or registered, and demand for it has increased, traditional healers are however challenged because they seldom have the capacity to produce in bulk, while maintaining quality. Large scale commercial production of validated herbal medicine requires professional management and presentation skills, which individual practitioners currently lack, although they may have access to sufficient supplies to meet the demand. In some cases, deteriorating quality has been noted, pointing to the need to establish linkages with local industries to invest in large- scale, consistent quality production. Lack of entrepreneurship skills, including in marketing, packaging and record keeping, also results in limited economic benefit for the traditional healers and may lead to a reluctance to share information with whoever can commercialise their products. In addition, potential investors stay away from commercial traditional medicine production and distribution, because of the absence of the necessary policy framework, leaving traditional healers with limited avenues to access funds. An appropriate policy environment would help in attracting investors interested in joint ventures, with better prospects for profitability for all concerned.
Accessible research, resources and documentation – Research funding is limited in Uganda, and this poses particular challenges in the field of traditional medicine, given the high costs involved (up to U.shs. 40 million per specimen). Validation requires time, specialised and costly testing equipment, with spares that cannot be obtained locally. Sending samples for testing to other countries is also expensive. Neither is NCRL in a position to provide substantial financial support to healers because of its own financial constraints. Having formal relationships is also held back by NCRL’s current legal status, although this is likely to change in the near future, when it will be allowed to enter into formal partnerships with associations of traditional healers. Further, the sample analysis work carried out at NCRL can only guide other agencies, such as the National Bureau of Standards and the Export Promotion Board to give additional assistance to healers. Limited resources slow down validation, to the disappointment of some healers. Patrick Ogwang, NCRL pharmacist and researcher, therefore observes that, while much useful knowledge exists among healers, the demand for validation far exceeds the capacity of the Laboratory and there are many pending applications. After testing, reports also need to be simplified so that healers can fully understand the results in terms of toxicity, safe dosage, appropriate administration and storage. With limited research, analysis and documentation, negative attitudes towards embracing traditional herbal medicine as a resource are not dispelled. The benefits of establishing and maintaining linkages between traditional medicine practitioners and modern medical institutions are then difficult to promote. Where advances have been made with this type of collaboration, the benefits and challenges of mainstreaming into modern medical practice also need to be analysed and documented, so that development actors identify areas for intervention and how traditional knowledge may complement their initiatives.
Conclusions and recommendations
With many of us returning to nature for health and nutritional remedies, a linkage between traditional healers and NCRL presents opportunities from which we all stand to benefit. These benefits could be diverse: the traditional practitioner can gain from sales and his clients from his contribution to primary health care. The Ministry of Health can benefit from savings on imported medicines, and from improved access and quality of herbal medicine for all. The economy can benefit from exports of Ugandan herbal medicine and from gainful employment for smallholder farmers cultivating medicinal plants on a commercial basis. This would help both public and private sectors to see traditional medicine and practice as a resource that can be harnessed, professionalized and turned into commercial gain. Further, collective efforts to promote traditional medicine will not only generate economic and health benefits, but also restore a sense of pride in an important part of our cultural heritage.
Recommendations
Legal framework. The establishment of the National Council of Indigenous and Complementary Medicine Practitioners or its equivalent must now be expedited so that a policy framework facilitates collaboration, funding, validation and the development of traditional medicine. Aspects that deal with intellectual property rights and patenting need enforcing and traditional practitioners informed about its provisions and implications, to help them feel freer to share their knowledge.
Policy implementation. With a wealth of biodiversity and indigenous knowledge, Uganda has the potential to develop traditional medicine into a valuable resource. The traditional healers’ contribution to health care in particular needs to be recognised by providing funds, facilitating fora where they can discuss their concerns, and referring the public and other stakeholders to them. This includes using the Traditional Medicine Day to promote herbal products and their use in the prevention and management of disease. Adequate resources must be allocated and linkages created to facilitate the implementation of plans to improve the quality, volume and sustainability of herbal medicinal production and use.
Nationwide comparative research, documentation and cost benefit analyses of using traditional medicine are needed to improve their usage. This requires expanded facilities at NCRL and the creation of regional research and testing laboratories, as well as simplified and decentralised validation and registration processes to encourage traditional practitioners to register their products. The promotion of herbal medicine could be included in the terms of reference of Community Development and District Health officers to facilitate their identification, the verification of their effectiveness and to establish the potential for commercial production. This would also help to institutionalise district-level health partnerships: a Private-Public partnership health desk in every district could host centralised and district information on health resources, including indigenous knowledge. Research findings on the value of traditional medicine could be disseminated via the popular mass media, including radio stations and video halls.
Enhancing economic value. The commercialisation of herbal medicine should be promoted, and its economic benefits to individual herbalists and the general public highlighted as a means to poverty reduction at household and national levels. Clear memoranda of understanding need to be developed to put the traditional healers’ expectations into perspective and allow them to negotiate from the onset the benefit they expect from partnership with other parties, including Government. They also need to be equipped with skills to manage the commercial production and sale of validated medicine, or to link them with public and private organisations that can enhance their services and products for commercial use.
Environment conservation. Aspects of environmental sustainability need to be incorporated in commercial herbal medicine promotion and the establishment of herbal gardens encouraged, especially for rare medicinal plant species. Availing land for research and for private sector commercial production would contribute to environmental conservation, in addition to health benefits.
Education and knowledge. Uganda needs to invest in curriculum development, training and capacity building to sustain existing knowledge and to promote new knowledge through formal and informal education at various levels – community sensitisation, as well as primary, secondary, and tertiary education. NCRL needs to respond to the call from the National Curriculum Development Centre to help incorporate traditional healers’ knowledge into the relevant educational curricula.
Here the French summary
Plus de la moitié de la population ougandaise pratique la médecine traditionnelle, un fait tout d’abord signalé en 1999 par la Politique nationale en matière de santé et considéré comme un apport considérable au système élémentaire de soin. La collaboration entre le gouvernement et le sous-secteur de la médecine traditionnelle et complémentaire est arbitrée par le Laboratoire de Recherche en Chimiothérapeuthiques Naturels (NCRL) sous la tutelle du ministère de la Santé afin de promouvoir et de préserver la médecine traditionnelle.
Cette étude de cas montre que, même si les bénéfices à approfondir cette relation sont incontestés pour tous les acteurs concernés, un certain nombre de contraintes demeure. Cela inclut notamment des coûts relativement élevés de production et de préparation pour les praticiens traditionnels alors que le soutien financier et l’encadrement offerts restent limités. Ces entraves, en partie dues à une législation surannée, restreignent l’engagement d’autres acteurs à valider, promouvoir et investir dans l’usage et la production commerciale de plantes médicinales, à réglementer la pratique des praticiens traditionnels et à fournir ainsi un contrôle de qualité effectif. Une connaissance limitée du brevetage et des droits de propriété intellectuelle amène également les guérisseurs à résister à divulguer leur savoir médicinal ; ceci est amplifié par une activité de recherche, d’analyse et de documentation limitée sur les intérêts des plantes médicinales, ce qui vient, à son tour, alimenter une vision négative et une réticence à envisager les plantes médicinales comme une ressource importante.
Ce cas met par conséquent en exergue un certain nombre de préconisations :
le cadre juridique doit être consolidé afin de faciliter la collaboration, la subvention, la validation et le développement de la médecine traditionnelle. Il est nécessaire que les droits de propriété intellectuelle et le brevetage soient respectés et que les praticiens traditionnels soient informés des dispositions d’ordre public et de leurs incidences afin d’atténuer leur inquiétude à partager leurs connaissances.
Le concours des guérisseurs traditionnels à la médecine doit être reconnu et récompensé par des financements, en rendant possible un forum où ils pourraient exprimer leurs préoccupations et en les recommandant au public. Des moyens satisfaisants devraient être attribués (ou les liens nécessaires créés) afin de faciliter la mise en œuvre des plans d’amélioration de qualité, de volume et de viabilité de la production et de l’utilisation de plantes médicinales.
Des recherches comparatives d’envergure nationale ainsi que des analyses coûts-avantages dans l’utilisation de la médecine traditionnelle sont également requises. Il conviendrait de promouvoir la commercialisation des plantes médicinales, de valoriser les bénéfices économiques pour les herboristes en tant que particuliers sans oublier de souligner l’intérêt général. Les praticiens traditionnels se doivent d’être dotés des compétences financières au regard de la production commerciale et de la vente des remèdes validés.
Les aspects relatifs à la gestion durable de l’environnement doivent être intégrés à la promotion commerciale des plantes médicinales et la création de jardins des plantes, notamment pour les espèces rares de plantes médicinales, encouragée.
L’Ouganda doit investir dans l’élaboration de programmes, dans la formation et dans le développement des compétences afin de pérenniser un savoir déjà existant et d’en promouvoir un nouveau grâce à une éducation tant informelle que formelle à différents échelons.
Avec le retour de bon nombre d’entre nous vers la nature en termes de produits de santé et de suppléments nutritionnels, un lien entre les guérisseurs traditionnels et le NCRL offre des opportunités dont nous pourrons tous bénéficier. Cela aiderait à la fois les secteurs public et privé à appréhender la médecine traditionnelle et sa pratique comme une ressource qui peut être exploitée, professionnalisée et convertie en but lucratif. En outre, les efforts conjugués pour promouvoir la médecine traditionnelle ne vont pas uniquement être profitables en termes de retombées pour l’économie et la médecine du pays, mais vont permettre également de restaurer un sentiment de fierté à l’égard d’une part importante de notre héritage culturel.
This is some how good but we need to saparate by aotonomising each by each sector to make a sane of meaning ot the two,traditional made cone should remain traditional madicing by improving it in its nature and remaining stand in its culture of that particular land and while developing it separetljy to have its recognition and if it needs to be developed let it have MOU between those deffarent developers and for uganda let the name of the council remain traditional medicine concil
A nice informative summary – I would like to start herbal plants gardens on my land to supply those who produce the medicines (this can have both medicinal and environment conservation benefits as usage of herbicides is turning certain medicinal plants into extinction). Which type of herbal plants have both medicinal and commercial value. Which varieties can I start with and what is the current demand and supply chain? I just have the interest.
Kiwanuka Benedict – 0772412814 (4 years training in agriculture, Masters Degree in Public Administration and Management, BA (SS) Degree in Economics and Political Science, Post Graduate Diploma in Education, Certificate in Social Business – Designing for Impact – African Management Institute Kenya (AMI)
Certificate in Planning, Management, Monitoring and evaluation of Community Development Projects – Uganda Management Institute.
Certificate in Preparation and Critical Appraisal of Project feasibility studies – Uganda Management Institute.
Certificate-Strategic Planning & Management Skills Improvement – Uganda Management Institute.
this is a nice piece which tries to clearly identify those underlying strategies which can be used to enhance the use tradition and complementary medicine in quite a more evidence based way.
I hope the gaps will soon be bridged between modern medicine and CAM, though more research work should still be done for a better improvement and reduction of the health service delivery burden in Uganda